Two conversations happening at once
When people talk about blue light and skin, they are usually talking about two different things without realising it. The first is whether screens and indoor LED lighting directly damage skin cells the way UV radiation does. The second is what blue light does to the body's circadian system and, through that, to the skin's overnight repair processes.
These are related but distinct questions. The evidence behind them is at very different stages of development. And the skincare industry has largely focused its marketing on the first question while the more compelling science, and the more relevant skin health concern, belongs to the second.
This article separates the two.
What blue light is
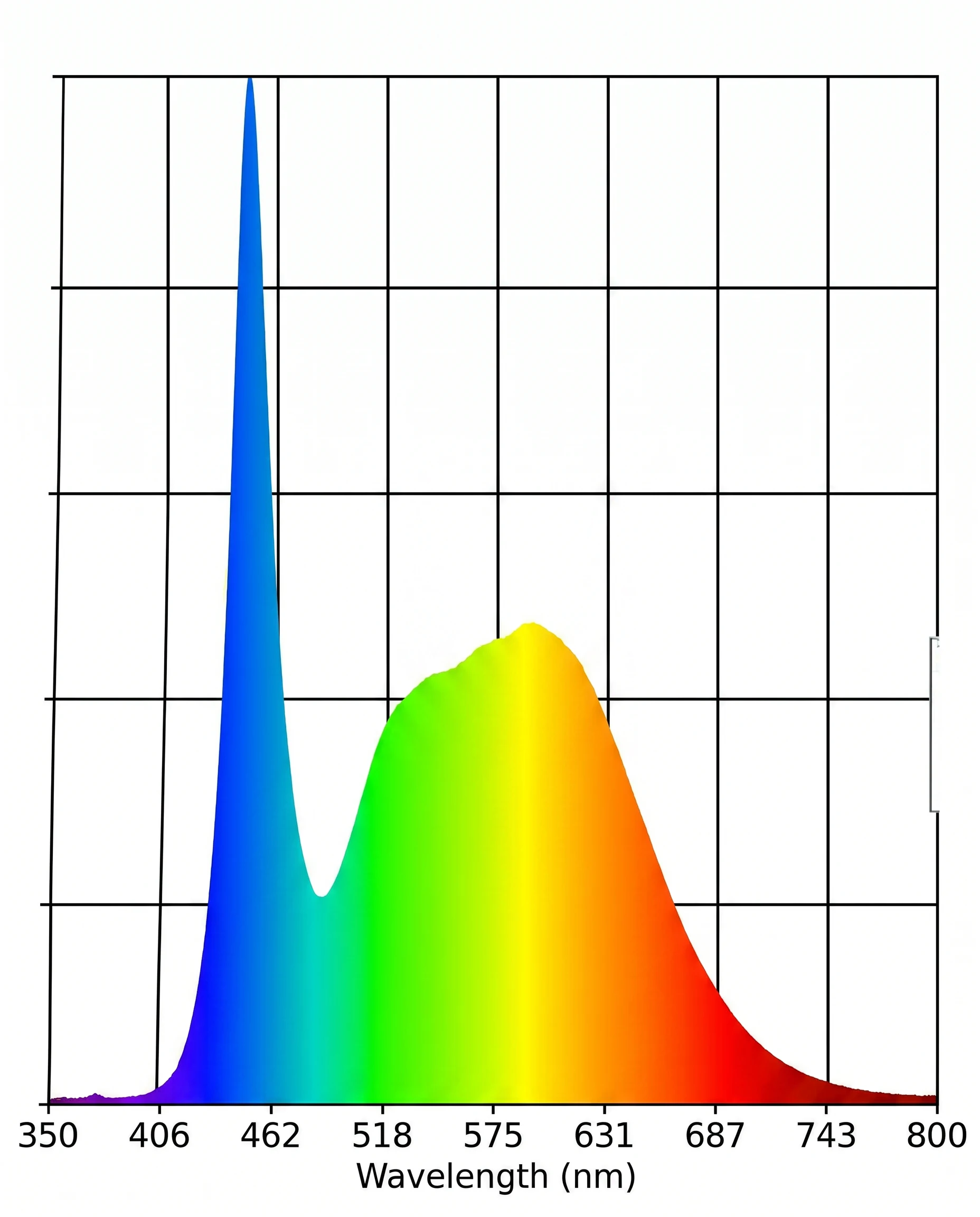
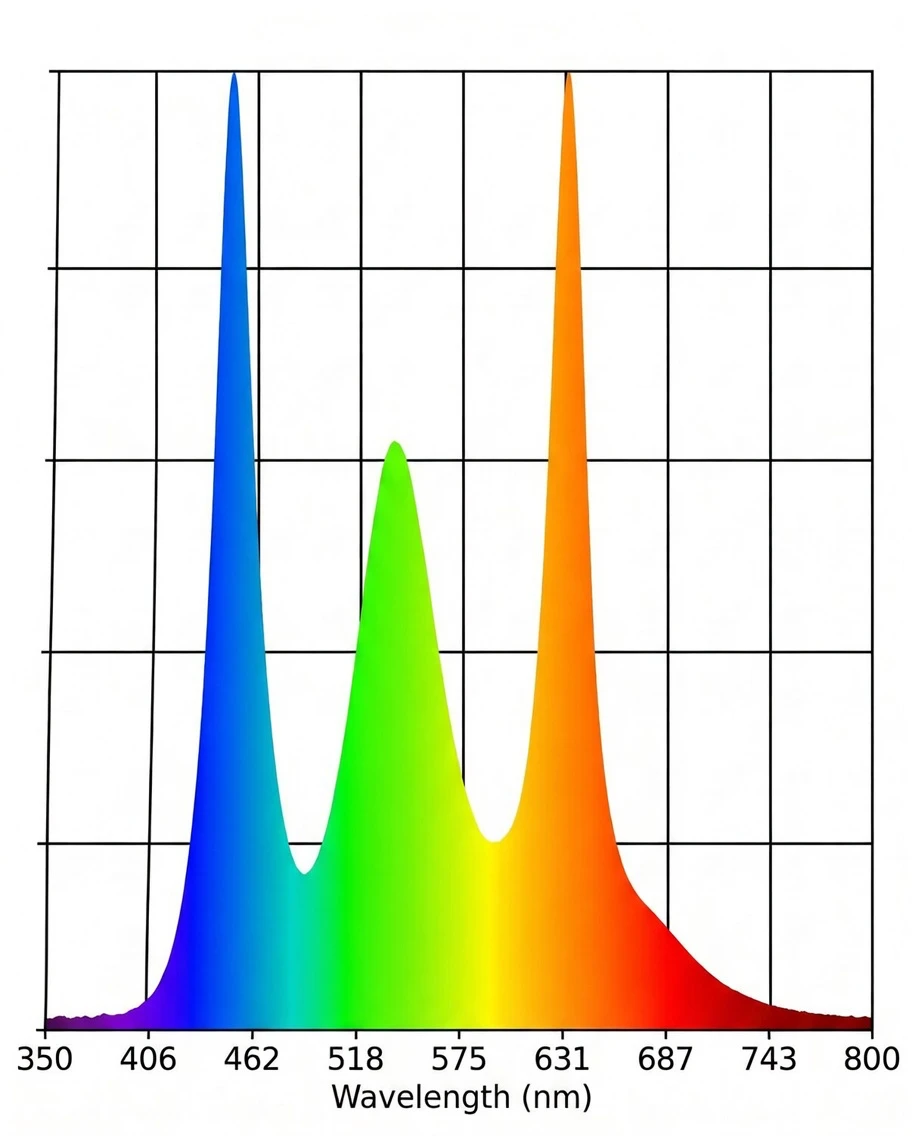
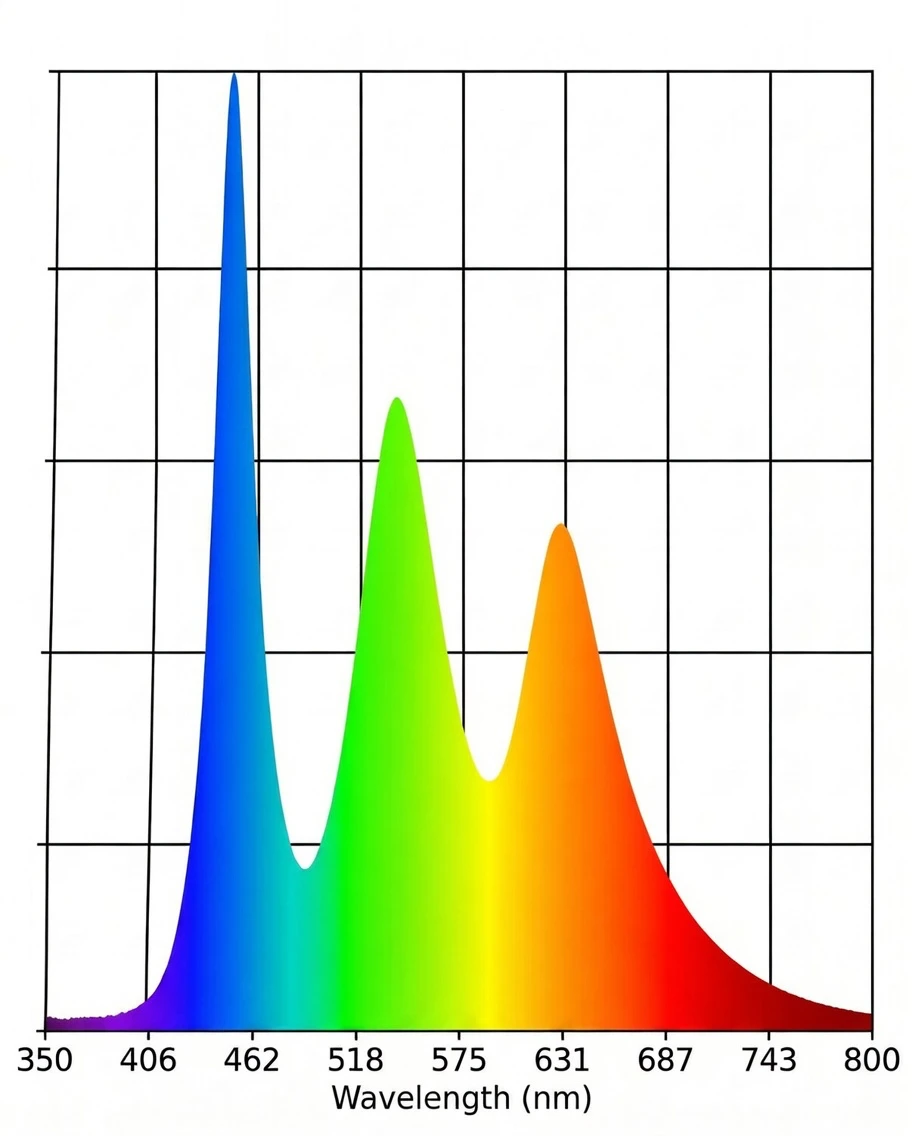
Visible light occupies the spectrum from roughly 380 to 700 nanometres. Blue and high-energy visible (HEV) light sits at the shorter, higher-energy end of that range, broadly from 400 to 500 nanometres, with the peak emission from screens and LED lighting typically falling around 440 to 460 nanometres.
For comparison: UVA runs from 315 to 400 nanometres and UVB from 280 to 315 nanometres. Both sit just beyond the visible range. The photons of UVB light carry more energy per photon than blue light photons, because energy increases as wavelength decreases. This is why UVB, even at lower doses, causes the DNA damage that leads to sunburn and skin cancer: the photons are energetic enough to directly break chemical bonds in DNA.
Blue light photons at 450 nanometres carry less energy per photon than UVB at 300 nanometres. This is a real physical difference and it matters for understanding the mechanism. But it does not settle the question of what chronic blue light exposure does to skin over years and decades, and it should not be used to do so.
The established mechanism: what blue light does to the circadian system
The most thoroughly documented effect of blue light on the body, and on skin specifically, is not direct photodamage. It is circadian disruption through melatonin suppression.
The eye contains a subset of retinal ganglion cells that are intrinsically photosensitive, meaning they respond to light independently of the rod and cone system used for vision. These cells contain the photopigment melanopsin, which is maximally sensitive to blue light at around 460 to 480 nanometres. When these cells detect light in this range, they signal to the suprachiasmatic nucleus, the brain's master clock, to suppress melatonin production by the pineal gland.1
The action spectrum for this suppression peaks squarely in the range produced by screens and modern LED lighting. Evening use of devices delays the natural rise of melatonin. It reduces the peak level reached during the night. And because melatonin is the hormonal signal that initiates the skin's overnight repair window, as covered in detail in What Does Melatonin Do in Skin Cells, this suppression has direct consequences for when and how efficiently skin repair runs.
This is not a hypothesis. It is one of the most replicated findings in chronobiology, documented across controlled trials, confirmed by spectral analysis, and the mechanistic basis for advice about limiting screen use in the evening. The problem with most "blue light skincare" content is that it has largely ignored this mechanism while focusing on the more photogenic but less settled story of direct skin cell damage.
The direct effects on skin cells: what the research shows and where it ends
In controlled laboratory conditions, HEV light has been shown to generate reactive oxygen species in skin cells, trigger oxidative stress, and activate melanin production in keratinocytes and melanocytes.2 At the irradiance levels used in phototherapy settings, these effects are measurable and meaningful. The research in this area is real and should not be dismissed.
The more complicated question is what happens at the irradiance levels people actually encounter indoors. A screen or an LED panel delivers a fraction of the photon dose of outdoor daylight, even on an overcast day. This is why acute comparisons between screen exposure and sun exposure, made without accounting for irradiance, are misleading.
What those comparisons miss, however, is cumulative dose over time. Modern indoor life means eight, ten, sometimes twelve hours per day of blue-weighted light exposure, every day, for decades. There is no long-term epidemiological data on what that accumulation does to skin at the cellular level. Studies tracking people through twenty or thirty years of heavy screen use and measuring outcomes like collagen integrity, oxidative DNA damage, or barrier function do not exist yet. They would take a generation to produce.
The research on chronic low-level HEV exposure and long-term skin effects is genuinely unresolved. What we have is the mechanism: HEV light generates reactive oxygen species in skin cells under controlled conditions, and those same cells contain photoreceptors capable of responding to visible light independently of UV. The frequency and duration of blue light exposure in modern indoor life is unprecedented in evolutionary terms. Whether that exposure, accumulated over years and decades, produces measurable harm to skin that is distinct from other sources of oxidative stress is a question the current literature cannot answer. The mechanism makes it a serious question. Honesty requires leaving it there.
NAD+ depletion: where the two mechanisms converge
There is a point where the direct cellular effects of blue light and its circadian consequences meet, and it is worth understanding because it connects to the repair biology covered elsewhere in this journal.
When cells sustain DNA damage from any source, oxidative stress included, they activate enzymes called PARP proteins (poly ADP-ribose polymerases). PARP enzymes carry out DNA repair by synthesising chains of ADP-ribose, and the raw material for those chains is NAD+. A cell under sustained oxidative stress runs its PARP enzymes continuously, and in doing so depletes its NAD+ reserves.
NAD+ is not only a substrate for DNA repair. It is the essential cofactor for sirtuin enzymes, the family of proteins responsible for coordinating many of the circadian-gated repair processes that run overnight in skin. When NAD+ is depleted, sirtuin activity falls. The cellular machinery that should be running the overnight repair programme has less of the fuel it depends on.
Chronic blue light exposure, to the extent that it generates sustained oxidative stress in skin cells, may contribute to this depletion through the PARP pathway. Circadian disruption from blue light at night reduces the melatonin signal that helps synchronise sirtuin activity. Both routes arrive at the same place: a reduction in the cellular resources available to run overnight repair. The companion piece on niacinamide in this journal covers what that means for NAD+ replenishment specifically.
What blue light blocking products actually claim
The marketing category that emerged around blue light in skincare primarily argues one of two things: that mineral filters in SPF products physically scatter or absorb HEV light before it reaches skin, or that antioxidant ingredients neutralise the oxidative damage blue light causes.
The first claim is technically accurate in a narrow sense. Zinc oxide and titanium dioxide do scatter some visible light. Whether the amount scattered from a typical SPF application provides meaningful protection against indoor blue light exposure is a different question. The geometry of indoor light is diffuse and surrounds you from multiple directions. A filter applied to the face provides no protection from the light falling on the rest of the body, the light reflected from surfaces, or the light entering through the eyes, which is where the circadian mechanism operates. Physical filtering on the skin cannot address the primary documented mechanism of harm.
The second claim, antioxidant protection, is more defensible but less specific than the marketing implies. Antioxidants do reduce oxidative stress in skin. They do this regardless of whether the oxidative stress originates from UV, blue light, metabolic processes, or environmental pollution. Framing general antioxidant activity as blue-light-specific protection is accurate only in the same sense that a seatbelt protects against car accidents caused by rain: true, but the rain is not really the point.
What this means in practice
The primary actionable concern from blue light and skin is not the one most blue light products are designed to address. It is the suppression of melatonin in the evening and the consequent disruption to the skin's overnight repair window. That cannot be fixed by a topical product. It is addressed by managing the timing and spectrum of light exposure, particularly in the two to three hours before sleep.
The potential cumulative effect of chronic HEV exposure on skin cells is a question the science has not settled. Given the mechanism and the unprecedented duration of modern indoor light exposure, it deserves to be taken seriously rather than dismissed on the basis of acute irradiance comparisons. General antioxidant support for skin is reasonable and consistent with the direction the evidence points, even if the specific blue-light framing overstates what is proven.
The circadian argument is where the evidence is strongest and where the gap between what the science shows and what the skincare industry addresses is widest. That gap is the subject of the next article in this journal.
- Blue and high-energy visible (HEV) light occupies 400 to 500 nanometres. UVB photons carry more energy per photon than blue light photons. This makes acute irradiance comparisons between screens and sunlight misleading in one direction, but does not settle the question of cumulative chronic exposure.
- The most thoroughly established effect of blue light on skin health is circadian disruption via melatonin suppression. Melanopsin-containing retinal ganglion cells respond maximally to light at 460 to 480 nanometres, the range produced by screens and LED lighting. Evening exposure delays and reduces melatonin onset, disrupting the hormonal signal that initiates skin's overnight repair window.
- Laboratory studies confirm that HEV light generates reactive oxygen species in skin cells and can affect melanin synthesis. At phototherapy intensities these effects are measurable. The cumulative effect of chronic low-level indoor HEV exposure over years and decades has not been studied longitudinally and the evidence is genuinely incomplete.
- DNA damage and oxidative stress activate PARP enzymes, which consume NAD+ during repair. Sustained oxidative stress from any source, including potentially chronic HEV exposure, may deplete NAD+ and reduce the sirtuin activity needed to run overnight skin repair.
- Physical blue light filtering in topical products cannot address the primary documented mechanism, which operates through the eyes and the circadian system. General antioxidant support is reasonable but is not specifically a blue light intervention.
- The circadian mechanism, not direct photodamage, is where the strongest evidence lies and where the largest gap exists between what the science shows and what the skincare industry currently addresses.
- Brainard GC, Hanifin JP, Greeson JM, et al. Action spectrum for melatonin regulation in humans: evidence for a novel circadian photoreceptor. J Neurosci. 2001;21(16):6405–6412.
- Liebmann J, Born M, Kolb-Bachofen V. Blue-light irradiation regulates proliferation and differentiation in human skin cells. J Invest Dermatol. 2010;130(1):259–269.